Model name: PRoGReSs (Hepatitis B model) - in VIMC until 2020
Modellers: Homie Razavi, Devin Razavi-Shearer
Institution: Center for Disease Analysis Foundation (CDAF)
The PRoGReSs Model is a dynamic model that quantifies the HBV-infected population by year, disease stage, sex, and age. The model also quantifies the susceptible population by the aforementioned categories with the exclusion of disease stage. The PRoGReSs model is designed to assess the impact of different strategies composed of any combination of perinatal prophylaxes (birth dose, three dose, hepatitis B immune globulin, and antiviral treatment of mothers) and/or the treatment of the population in reducing the burden of hepatitis B virus in a country.
The model utilizes inputs that are available for most countries in the literature to compute the size of the HBV-infected population – hepatitis B surface antigen (HBsAg) prevalence, hepatitis B e antigen (HBeAg) prevalence, population, background mortality by age/sex, and current/past vaccination rates. The model estimates perinatal transmission, non-perinatal transmission, and disease progression by calibrating to empirical data – prevalence by age and hepatocellular carcinoma (HCC) incidence and core antibody prevalence.
Razavi-Shearer, D., Gamkrelidze, I., et al. Global prevalence, treatment, and prevention of hepatitis B virus infection in 2016: a modelling study. Lancet Gastroenterol Hepatol 2018; 3(6): 383–403.
Model name: Hepatitis B model
Modellers: Tim Hallett, Margaret de Villiers, Shevanthi Nayagam
Institution: Imperial College London
The model is a dynamic, deterministic mathematical transmission model of the global hepatitis B epidemic structured by age, sex, and region. The model is composed of 21 Global Burden of Disease world regions, and is fitted to data on hepatitis B surface antigen (HBsAg) and hepatitis B e antigen (HBeAg) prevalence, at two time points, and liver cancer deaths for each region independently.
The model incorporates region-specific demographic data on population size, mortality, and fertility schedules, coverage of existing interventions (infant vaccination, birth-dose vaccination, and treatment availability), and assumptions about the natural history of HBV. In the model, mother-to-child transmission, transmission between children, and transmission across the whole population (which includes other forms of transmission including sexual and iatrogenic) are included, the relative strengths of which are inferred through the calibration procedure.
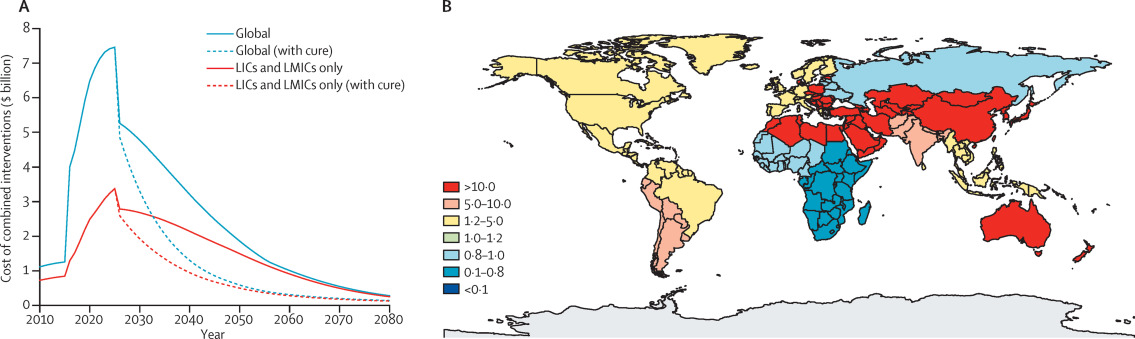
Cost of combined interventions and ratio of HBV and HIV treatment need.
(A) Cost of combined interventions with and without cure. The solid lines represent the cost of the combined interventions in the absence of a cure. The dotted lines represent the costs with the introduction of a cure in 2025. The blue lines represent the total global cost. The red lines represent the costs incurred in LICs and LMICs only (as defined by the World Bank in 201430).
(B) Ratio of people requiring treatment for HBV (modelled estimates for 2025) to people requiring treatment for HIV (HIV estimate from UNAIDS 201331). HBV=hepatitis B virus. LICs=low-income countries. LMICs=lower-middle-income countries.
From Nayagam, S., Thursz, M., Sicuri, E., Conteh, L., Wiktor, S., Low-Beer, D. L., & Hallett, T. B. (2016). Requirements for global elimination of hepatitis B: a modelling study. Lancet Infectious Diseases, 16(12), 1399-1408. Licensed under a Creative Commons Attribution License
Model name: Hepatitis B model
Modellers: Xi Li
Institution: Independent
The model was developed by Susan T Goldstein and colleagues at Centers for Disease Control and Prevention (CDC). It is a deterministic model of global hepatitis B burden. The age- and region-specific risk of developing acute and chronic hepatitis B infection was determined by the prevalence of hepatitis B virus seromarkers in early childhood and at the age of peak prevalence reported in literature and serosurvey reports. The risk of death from cirrhosis and hepatocellular carcinoma was derived from death registries, cancer registries and cohort studies in multiple countries. The lives that are saved by hepatitis B vaccine is calculated as the difference between predicted deaths from hepatitis B in an unvaccinated cohort and a vaccinated cohort, the latter based on the vaccination coverage of the cohort and assumptions on vaccine efficacy.
Goldstein, S. T., Zhou, F., Hadler, S. C., Bell, B. P., Mast, E. E., & Margolis, H. S. (2005). A mathematical model to estimate global hepatitis B disease burden and vaccination impact. Int J Epidemiol, 34(6), 1329-1339.